Beyond Telemedicine: Detecting Cervical Cancer in Amazonian Leticia, Colombia
By Luisa Orozco, our correspondent in Leticia
Leticia, the capital of the Colombian department of Amazonas, has an estimated population of 50,000 people, a significant proportion of whom are Indigenous. Nearly half of the population are women. Located at the tri-border region where Colombia, Brazil, and Peru meet, Leticia occupies a strategically and socially complex territory shaped by geographic isolation, cross-border mobility, and longstanding structural inequalities.

The city is difficult to access. It has no road connections to the rest of the country, and travel largely depends on air and river transport. This isolation has profound implications for healthcare access. In the region, barriers to medical care intersect with broader dynamics such as drug trafficking, human trafficking, illegal mining, and the historical neglect of peripheral and Indigenous communities. Together, these conditions create an environment in which preventive healthcare is often fragmented, delayed, or altogether inaccessible.
One of the major public health concerns affecting women in these settings is infection with human papillomavirus (HPV), a group of more than 200 related viruses, some of which are transmitted through sexual contact. HPV is extremely common, and most sexually active individuals are exposed to it at some point in their lives. While many infections resolve on their own, persistent infection with certain high risk strains can lead to several forms of cancer, including cervical cancer, which remains one of the most preventable yet deadly cancers affecting women globally.
In Leticia, the healthcare system faces serious limitations. The city hosts the main referral center for the department, a secondary level hospital that lacks high complexity care and specialized oncology services. As a result, women requiring more advanced diagnostics or treatment often need to be transferred to major urban centers such as Bogotá, which can involve long travel times, high costs, and delays that place continuity of care at risk.
In response to these structural gaps, health brigades organized by social organizations and the military have become an important mechanism for extending healthcare access into underserved communities. These brigades provide a range of services, including general medicine, pediatrics, psychology, dentistry, and sexual and reproductive health care. Within this framework, cervical cancer screening has become a particularly critical intervention.
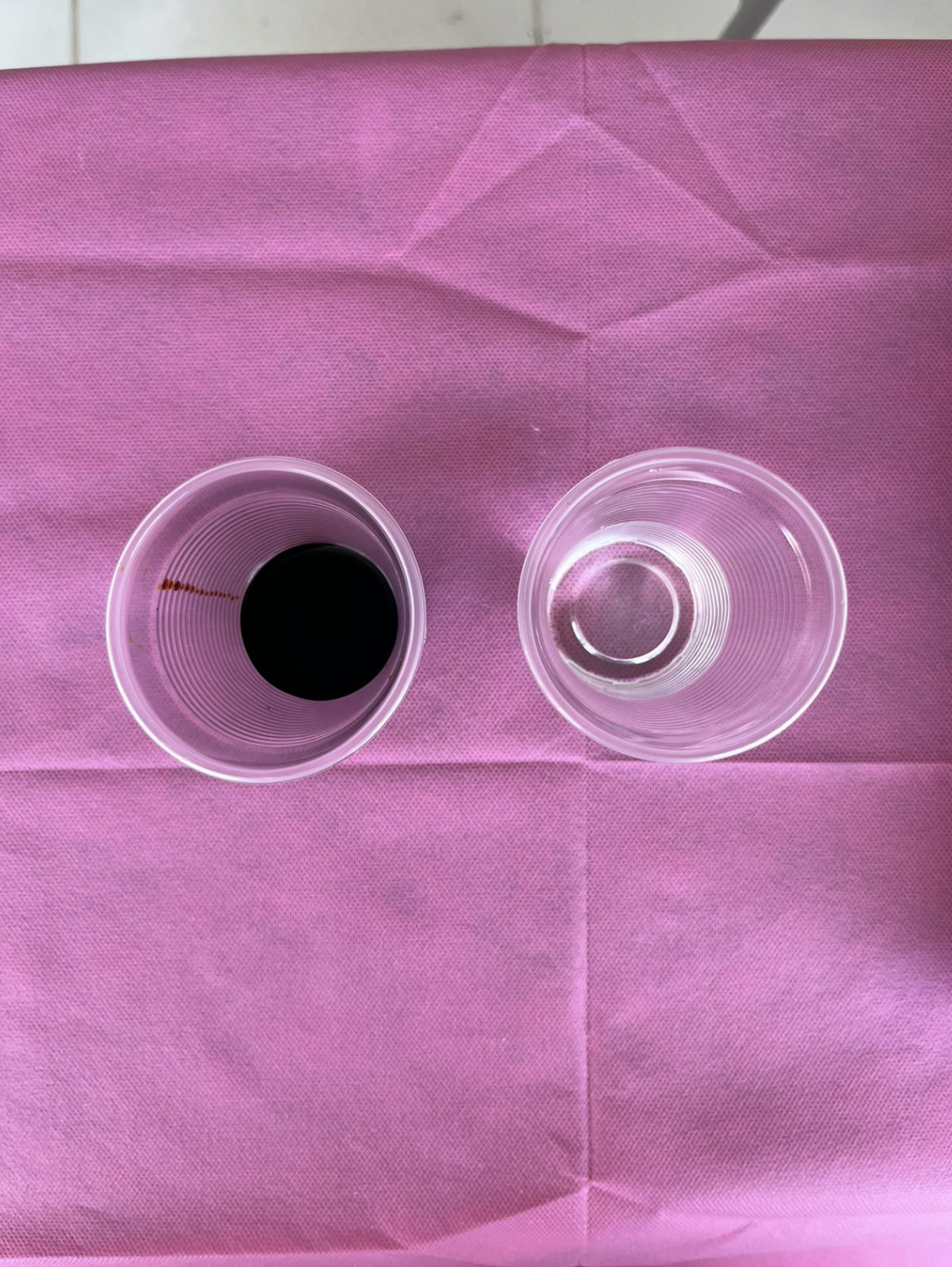
One of the main screening strategies used in these contexts is visual inspection with acetic acid (VIA), a low cost method especially suited to rural and hard to reach areas. VIA involves applying acetic acid and, in some cases, Lugol’s iodine to the cervix in order to highlight abnormal tissue changes that may indicate precancerous lesions. Unlike cytology based methods such as the Pap smear, VIA can be performed with minimal infrastructure and produces results almost immediately.
This immediacy is one of its greatest strengths. In contexts where patients may only have a single opportunity to access care, same day screening and counseling can significantly reduce loss to follow up. According to nurse Jessika Bermúdez, who has participated in multiple health brigades in rural Colombia, VIA is particularly effective in low resource settings because it requires only basic materials and can be deployed in communities where laboratory capacity is absent or severely limited.


Crucially, the presence of lesions does not mean a person has cancer. Many cervical abnormalities are reversible and highly treatable when detected early. However, a positive VIA result still requires follow up within the healthcare system, including procedures such as cryotherapy or thermal ablation to remove or treat abnormal tissue before it progresses.
Cervical cancer generally develops over several years, which makes prevention and early detection especially effective tools for reducing mortality. Yet in settings like Leticia, the challenge is not only medical. It is also educational, logistical, and structural. Many women continue to face fear, stigma, and misinformation around HPV and cervical screening. A positive result is often immediately associated with a cancer diagnosis, reinforcing anxiety and deterring care seeking.
As Bermúdez explains, this is where health education becomes essential. Increasing community understanding of what HPV is, how common it is, and how treatable cervical lesions can be when identified early is key to improving outcomes. In remote Amazonian contexts, strengthening regular screening efforts must go hand in hand with culturally responsive communication, trust building, and investment in sustained follow up care.
The case of Leticia illustrates a broader challenge across remote and marginalized regions: ensuring that early detection strategies are not only available, but meaningfully integrated into systems of care that women can actually access. In these contexts, methods such as VIA are not simply technical alternatives. They are critical tools for addressing preventable inequities in women’s health.